Published on May 24, 2022

Increased sunlight (not just UVB) is related to reduced COVID-19 disease transmission, severity, and a lower risk of death
Key Points
- A study found seasonal and daily fluctuations with significant variability in immune cell counts and CRP levels, with changes directly related to the length of day
- Several studies have found a correlation between increased duration of sunlight exposure and a better COVID-19 recovery rate, as well as a link between latitude and COVID-19 fatality rate with countries closer to the equator having lower fatality rates
- UVB, UVA, and even violet rays from sunshine have been shown to inactivate the SARS-CoV-2 virus itself, however, the time it takes for each to do so varies based on latitude, season, and time of day
 The incidence of infectious disease has been related to several factors, including season, temperature, humidity, and UV radiation, with certain respiratory and other illnesses being especially known to increase during specific months or seasons. For example, October is generally the month when we start to see an increase in cold and flu activity, with most respiratory virus and flu activity peaking between December and March. Meanwhile, polio is usually increased in summertime, and relapses in autoimmune diseases have also been found to be seasonal.
The incidence of infectious disease has been related to several factors, including season, temperature, humidity, and UV radiation, with certain respiratory and other illnesses being especially known to increase during specific months or seasons. For example, October is generally the month when we start to see an increase in cold and flu activity, with most respiratory virus and flu activity peaking between December and March. Meanwhile, polio is usually increased in summertime, and relapses in autoimmune diseases have also been found to be seasonal.
Seasonal variations are seen at the cellular level as well. Wyse et al. looked at seasonal and daily fluctuations in immune cell counts, and found both daily and seasonal patterns with significant variability. Neutrophil counts peaked in January with a low in July, and lymphocytes peaked in March with a low in October. Daily variation was seen for all white blood cells, with counts lowest early in the morning and increasing throughout the day. Seasonally, CRP levels were higher in the winter with a peak in December and a low in July. These changes were related to the length of day, with the most susceptibility to infectious disease occurring during the resting phase (night time) of the daily cycle.
Could Season and Sunshine have an Effect on COVID-19?
Several studies have found a correlation between increased duration of sunlight exposure and a better COVID-19 recovery rate, as well as a link between latitude and COVID-19 fatality rate with countries closer to the equator having lower fatality rates. This diagram by Sharun et al. illustrates the potential impact of sunlight on COVID-19 transmissibility, morbidity, and mortality.
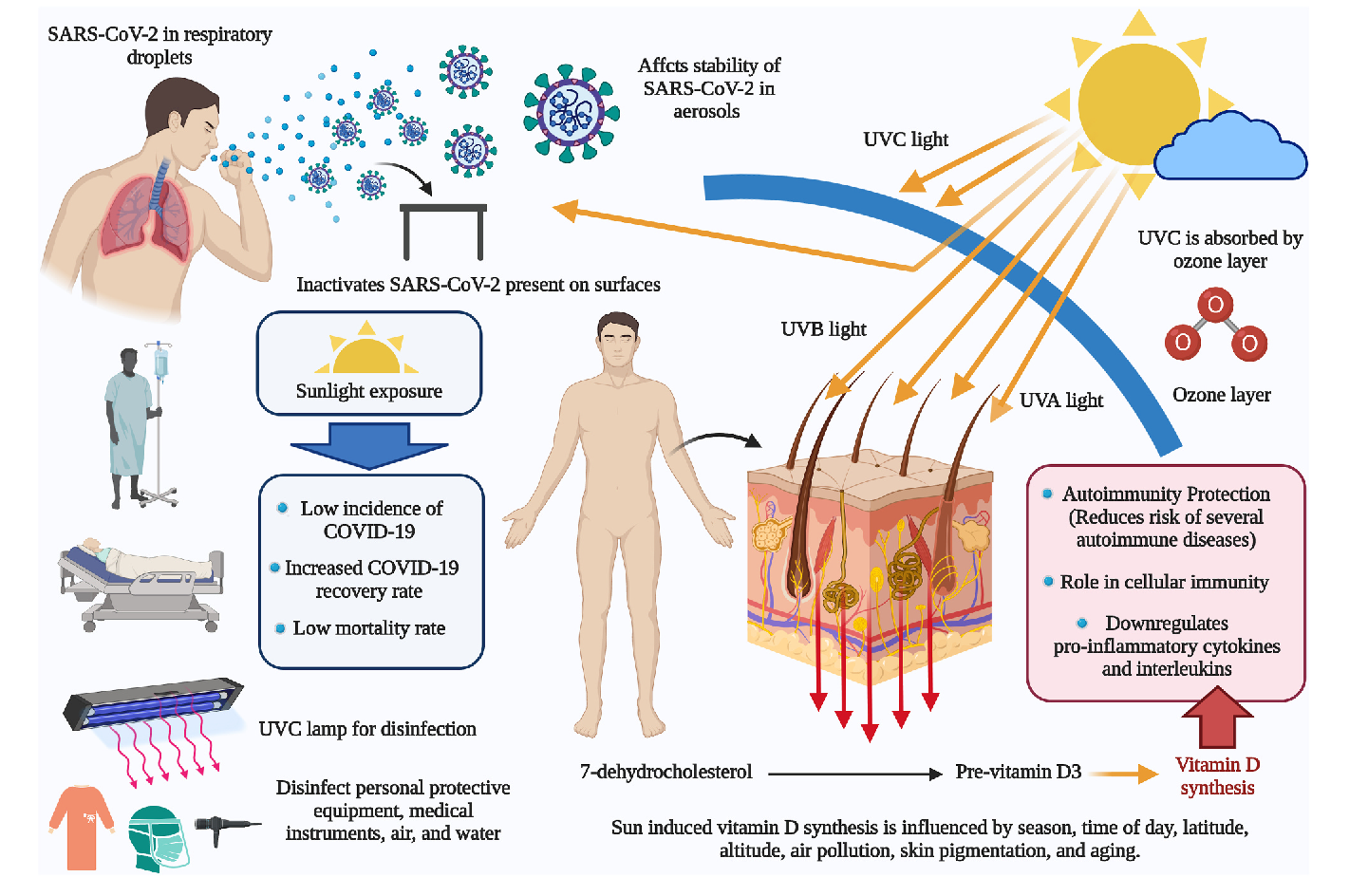
The authors of this review conclude “… based on the available data, the incidence, mortality, and recovery rate in patients with COVID-19 is considered to be correlated with sunlight exposure and vitamin D levels.” While vitamin D levels are significantly linked to COVID-19 disease risk and outcomes, there are other factors resulting from sunshine exposure that are demonstrating a beneficial effect as well.
Increased Sunlight (not just UVB) Related to Reduced Disease Severity and a Lower Risk of Death due to COVID-19
A review by Gorman and Weller suggests that UV exposure may reduce viability of the SARS-CoV-2 virus, its rates of infection and replication, as well as disease severity, and that these effects are due to different wavelengths of light from sunshine. Their paper describes the anti-viral, anti-inflammatory, and cardiometabolic benefits offered by UV light specifically, due in part to the release of vitamin D upon exposure to UVB and nitric oxide upon exposure to UVA, which has benefits for cardiovascular and metabolic health. Specific cardiovascular and metabolic diseases, including high blood pressure and diabetes, have proven to be some of the main risk factors for severe COVID-19 disease and death due to COVID-19, meaning that UV exposure from sunshine or other devices may lead to improved outcomes from each cardiovascular, metabolic, and COVID-19 diseases.
A positive association between higher ambient UV levels and lower rates of COVID-19 death was seen in most of the studies reviewed, along with a relationship between a higher UV Index and lower rates of death from COVID-19, which could be explained by more UVB induced vitamin D production with the higher UV Index.
To look at the effects of UVA specifically, Cherrie et al. investigated the association between UVA exposure and death due to COVID-19 in particular areas of the United States, England and Italy. The authors only looked at data from locations that were experiencing a “vitamin D winter” – where UVB levels were too low to produce a significant amount of vitamin D during the time of the study – to reduce the potential confounding effect of vitamin D on the COVID-19 outcomes. This video by one of the study authors briefly summarized the study and its findings (increased UVA exposure correlated with less COVID-19 fatalities).
Daily average UVA exposure during the study time varied between countries. As shown in the charts below, when comparing UVA exposure to the COVID-19 mortality rates within each area studied, a reduction in mortality rate ratio (MRR) of 0.71 was seen for every 100 KJ/m2 increase in UVA in the US, a reduction of 0.81 in Italy, and a reduction of 0.49 in England. Overall, when all three countries were combined, there was a mortality rate ratio reduction of 0.68 for every 100 KJ/m2 increase in UVA, with a predicted decrease in average risk of death by one-third to one-half from the lowest level of UVA to the highest level in each country. In other words, increased sunlight (specifically non-UVB in this study) was related to a much lower risk of death due to COVID-19.
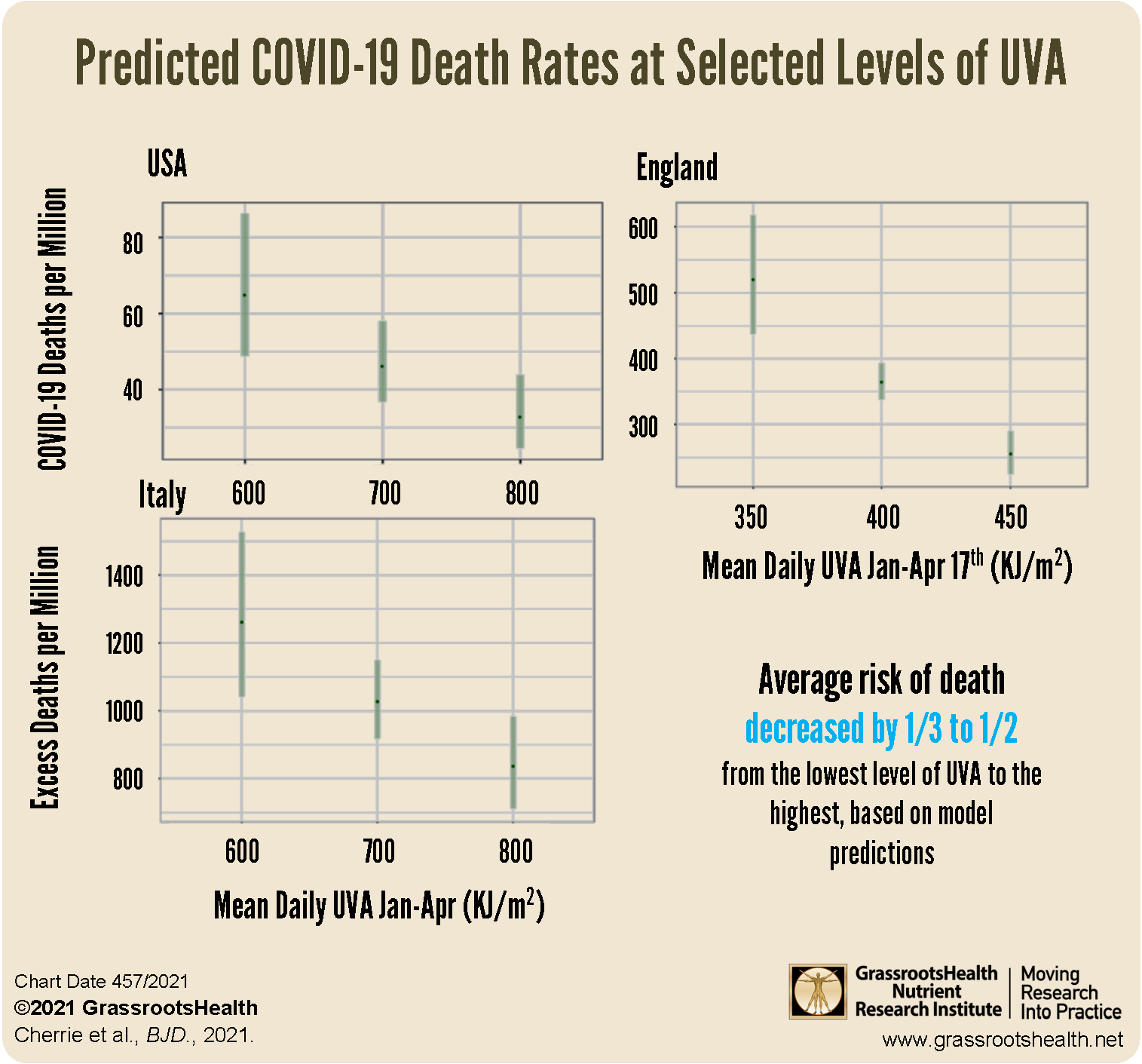
The authors of this study conclude that “optimizing sun exposure may be a possible public health intervention” independent of vitamin D… and, it’s free!
Could Sunshine Deactivate the SARS-CoV-2 Virus and Help Stop Transmission?
The above focuses mostly on the correlation between sunshine and/or UV exposure and COVID-19 disease outcomes among those who were already infected by the SARS-CoV-2 virus. Could sunshine help prevent the spread of viral infection before infection happens?
YES! UVB, UVA, and even violet rays from sunshine have been shown to inactivate the SARS-CoV-2 virus itself, however, the time it takes for each to do so varies based on latitude, season, and time of day.
One study by Ratnesar-Shumate et al. examined the effect of simulated sunlight on the activity of SARS-CoV-2 virus in either a simulated saliva or complete growth medium (gMEM). The researchers built a custom solar simulator that produced light in the ultraviolet (UV) range of 280-400 nm to best match natural sunlight, a range that contains both UVA and UVB wavelengths. Light intensity was controlled and adjusted to three different levels to imitate different times of day and year, with a UVB irradiance of 1.6 W/m2 (high sunlight intensity), 0.7 W/m2 (medium sunlight intensity), and 0.3 W/m2 (low sunlight intensity). Temperature and relative humidity were controlled for and monitored continuously.
The virus was added to either a simulated saliva solution or gMEM cell culture before being placed on a stainless steel surface, and allowed to dry for 30 minutes. Both were then exposed to the simulated sunlight for durations ranging from 2 to 18 minutes. The initial concentration of SARS-CoV-2 was 1:10, and viral concentrations were measured after each duration of exposure.
Inactivation of SARS-CoV-2 is charted as a function of UVB irradiance in the charts below. The rate of inactivation at any level of UVB irradiance was significantly faster when compared to the rate of inactivation in darkness (P<0.0001) – in fact, darkness had no significant effect on viral activity over the duration times studied, at a max of 60 minutes.
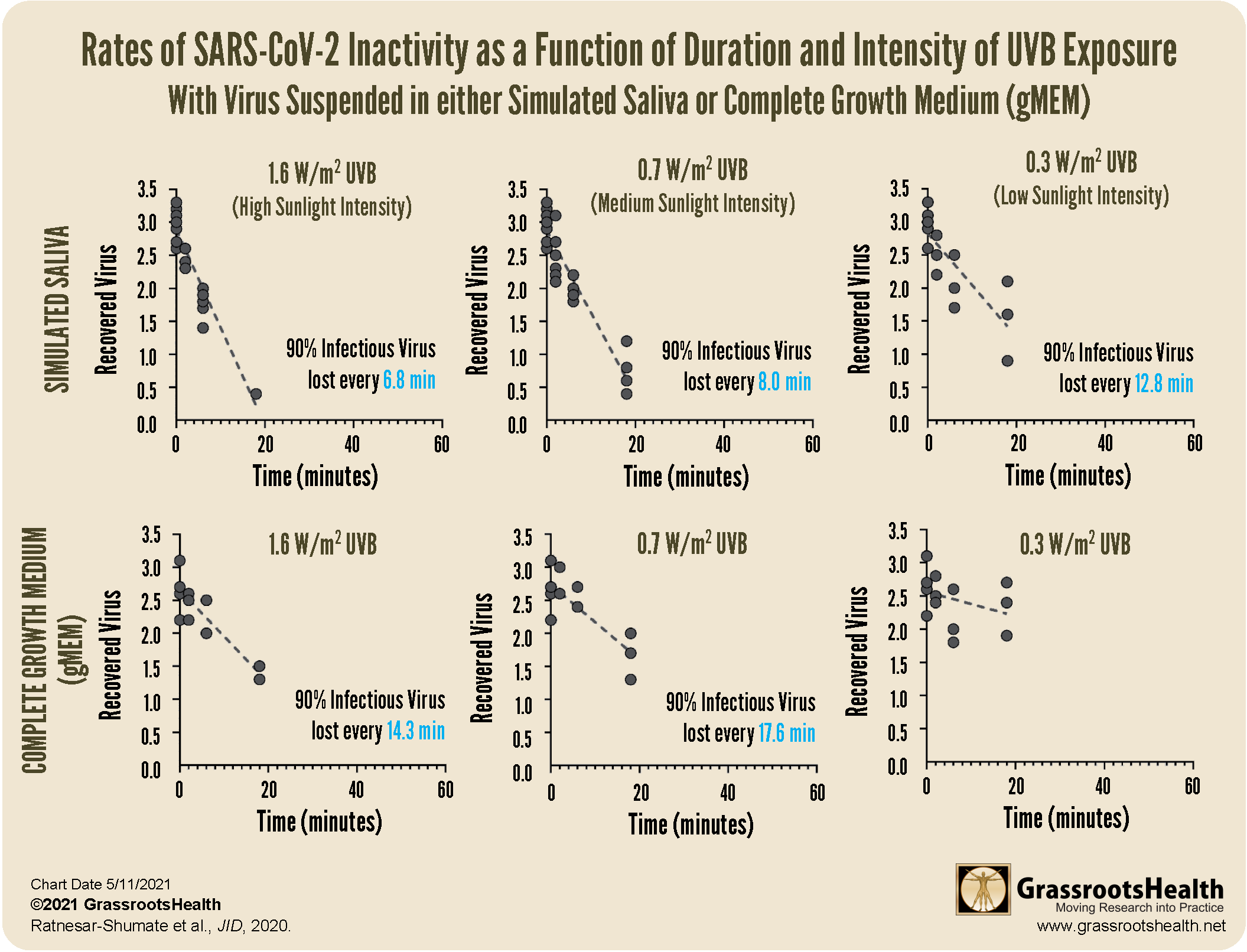
Overall, the study found that the inactivation rate of the virus was significantly associated with the amount of UVB irradiance and the suspension matrix. Compared to the lowest intensity UVB, the inactivation rate of the virus was much faster at the medium and high UVB levels. Based on analysis, ninety percent of the infectious virus would have been lost every 6.8, 8.0, and 12.8 minutes for high, medium, and low levels of UVB irradiance when in saliva, and 14.3 and 17.6 minutes for high and medium UVB irradiance when in the gMEM matrix.
Several other studies have demonstrated the solar-sensitivity of the SARS-CoV-2 virus. Biasin et al. found that the amount of SARS-Cov-2 virus in the sputum of COVID-19 patients can be completely inactivated by UVA and UVB wavelengths, blocking infectivity. While the dose of each wavelength varied, UVC (which does not reach the earth’s surface but can be used through devices), UVB, UVA, and violet light all resulted in viral inactivation over time.
Nicastro et al. also showed that UVA and UVB photons have powerful virucidal effects against the SARS-CoV-2 virus and other single-stranded RNA viruses. In particular, they found that “the Solar radiation that reaches temperate regions of the Earth at noon during summers, is sufficient to inactivate 63% of virions in open-space concentrations… in less than 2 min.” The authors describe the amount of time needed to inactivate the virus at noon for each degree of latitude during different months of the year, with a much greater monthly variation at the higher latitudes (representing seasonality).
A study by Rendell et al. looked at the ability of UV radiation in the United Kingdom to inactivate the SARS-CoV-2 virus. The authors found that, while certain months (April and May of 2020) did have higher amounts of UV available with the potential to have a significant impact (at least 90% viral inactivation), for 50-60% of the year (most of October through March) solar UV was not likely to have a significant impact – another representation of seasonality.
Overall, these studies provide evidence that increased sunlight may not only help reduce the risk of severe viral infections, but it may also be an effective disinfectant for SARS-CoV-2 and other viruses.
Sunlight and Vitamin D Could Reduce the Spread of Respiratory Viruses and COVID-19
Mukherjee et al. completed a meta-analysis to validate the relationship between low vitamin D levels and increased COVID-19 infection. They then used meteorological data to demonstrate the negative association between daily COVID-19 cases and temperature, UV Index, and cloud-free vitamin D UV doses, and concluded that “The findings of this study suggest that low UV exposure can affect the required production of vitamin D in the body, which substantially influences the dynamics of COVID-19 transmission and severity.”
A study by Schuit et al. showed the impact of simulated sunlight on aerosol transmission of the influenza virus, demonstrating an inverse relationship between simulated sunlight intensity and transmission of the influenza virus over long distances, regardless of humidity. This experimental study demonstrated nearly 100% viral decay after only 8 minutes of exposure to simulated sunlight, with a decay rate (of influenza virus) 13-times higher for sunlight compared to darkness.
Dr. Marc Sorenson, founder of the Sunlight Institute, commented on the Schuit et al. study, saying “The information from that simple paper is astounding… A decay rate (of influenza virus) 13-times higher for sunlight vs darkness is remarkable. It means instead of isolating at home, we need to either get out in the midday sunshine or get in a sunbed… Sunlight is the best disinfectant.” He continues by saying, “This is a beautiful thing, because internally, vitamin D can shut down the cytokine storm (inflammatory immune response), and externally, sunlight can cleanse the air. A great one-two punch.”
The same seems to be true for sunlight and COVID-19 as well!
Make Sure You are Getting Enough Vitamin D TODAY!
 Having and maintaining healthy vitamin D levels and other nutrient levels can help improve your health now and for your future. Choose which additional nutrients to measure, such as your omega-3s and essential minerals including magnesium and zinc, by creating your custom home test kit today. Take steps to improve the status of each of these measurements to benefit your overall health. With measurement you can then determine how much is needed and steps to achieve your goals. You can also track your own intakes, symptoms and results to see what works best for YOU.
Having and maintaining healthy vitamin D levels and other nutrient levels can help improve your health now and for your future. Choose which additional nutrients to measure, such as your omega-3s and essential minerals including magnesium and zinc, by creating your custom home test kit today. Take steps to improve the status of each of these measurements to benefit your overall health. With measurement you can then determine how much is needed and steps to achieve your goals. You can also track your own intakes, symptoms and results to see what works best for YOU.
Enroll in D*action and Test Your Levels Today!
How Can You Use this Information for YOUR Health?
Having and maintaining healthy vitamin D and other nutrient levels can help improve your health now and for your future. Measuring is the only way to make sure you are getting enough!
STEP 1 Order your at-home blood spot test kit to measure vitamin D and other nutrients of concern to you, such as omega-3s, magnesium, essential and toxic elements (zinc, copper, selenium, lead, cadmium, mercury); include hsCRP as a marker of inflammation or HbA1c for blood sugar health
STEP 2 Answer the online questionnaire as part of the GrassrootsHealth study
STEP 3 Using our educational materials and tools (such as our dose calculators), assess your results to determine if you are in your desired target range or if actions should be taken to get there
STEP 4 After 3-6 months of implementing your changes, re-test to see if you have achieved your target level(s)



