Published on August 9, 2022

How have you and those around you responded to the latest interpretation of the VITAL trial on fracture rates? Here is Part 1 of our 3-part response for you to share with others.
Key Points
- We know, beyond a doubt, that vitamin D is essential for our health; the “Totality of Evidence” provides the “whole-picture proof” that vitamin D can benefit our musculoskeletal, immune, cardiovascular, cognitive, and overall health, and reduces the risk of many diseases
- While randomized controlled trials (RCTs) are efficient ways to evaluate the effects of a drug (something that is not present in the human body unless taken), the RCT design is often not the best-suited study for nutrients; the fact is that many RCTs of nutrient effects are poorly designed, a reason they can tend to lead to a finding of “no effect,” or a “null” result, when in fact, with a different design, the findings could have told a much different story
- Robert Heaney, MD, who spent much of his career doing research on vitamin D and other nutrients, developed and published a paper outlining specific criteria nutrient studies should follow in order to produce the most accurate and reliable study results, which are especially important when it comes to vitamin D
 The latest publication from the VITAL trial, authored by LeBoff et al., titled “Supplemental Vitamin D and Incident Fractures in Midlife and Older Adults” has gotten everyone talking again about vitamin D. Articles with headlines such as “Is Vitamin D Overrated? Another Study Casts Doubt on Benefits” and “Study Finds Another Condition That Vitamin D Pills Do Not Help” led to confusion and doubt about the use of vitamin D supplements. Responses from practitioners who have written to us since the publication and the publicity that followed included “now I get people saying that vitamin D does not work” – imagine the damage this might be causing to people’s health when their translation of the headlines leads to ideas such as this!
The latest publication from the VITAL trial, authored by LeBoff et al., titled “Supplemental Vitamin D and Incident Fractures in Midlife and Older Adults” has gotten everyone talking again about vitamin D. Articles with headlines such as “Is Vitamin D Overrated? Another Study Casts Doubt on Benefits” and “Study Finds Another Condition That Vitamin D Pills Do Not Help” led to confusion and doubt about the use of vitamin D supplements. Responses from practitioners who have written to us since the publication and the publicity that followed included “now I get people saying that vitamin D does not work” – imagine the damage this might be causing to people’s health when their translation of the headlines leads to ideas such as this!
Looking at the Whole Picture First to Make Common Sense Conclusions
We know, beyond a doubt, that vitamin D is essential for our health. The “Totality of Evidence” provides the “whole-picture proof” that vitamin D can benefit our musculoskeletal, immune, cardiovascular, cognitive, and overall health, and reduces the risk of many diseases. Knowledge of human physiology has proven there is a demand for vitamin D within our cells for a multitude of every-day processes. Mechanistic studies have demonstrated how vitamin D works within the cells, tissues, organs, and the body as a whole to directly influence health and the development or regression of many skeletal and non-skeletal diseases. We see the effects of vitamin D demonstrated in observational and epidemiological studies over and over, with disease risk, prevalence, and outcome consistently related to vitamin D levels for many different types of diseases.
How Randomized Controlled Trials (such as VITAL) Fit in the Vitamin D Picture
In the medical science world, randomized controlled trials (RCTs) are considered the “gold-standard” study design to provide solid evidence that “something works.” Since there has been so much evidence and research supporting the role of vitamin D in health, researchers took what they thought was the next logical step to further clarify if and how vitamin D did have an effect on certain health outcomes – they designed and executed RCTs for vitamin D. Unfortunately, while RCTs are efficient ways to evaluate the effects of a drug (something that is not present in the human body unless taken), the RCT design is often not the best-suited study for nutrients. The fact is that many randomized controlled trials of nutrient effects are poorly designed, a reason they can tend to lead to a finding of “no effect,” or a “null” result, when in fact, with a different design, the findings could have told a much different story.
Let’s Tell the Story “Right” – Using Dr. Heaney’s Nutrient Study Criteria
To address issues arising from research such as this, Robert Heaney, MD, who spent much of his career doing research on vitamin D and other nutrients, developed and published a paper, “Guidelines for optimizing design and analysis of clinical studies of nutrient effects.” The table below lists the guidelines he recommended for optimum nutrient study design.
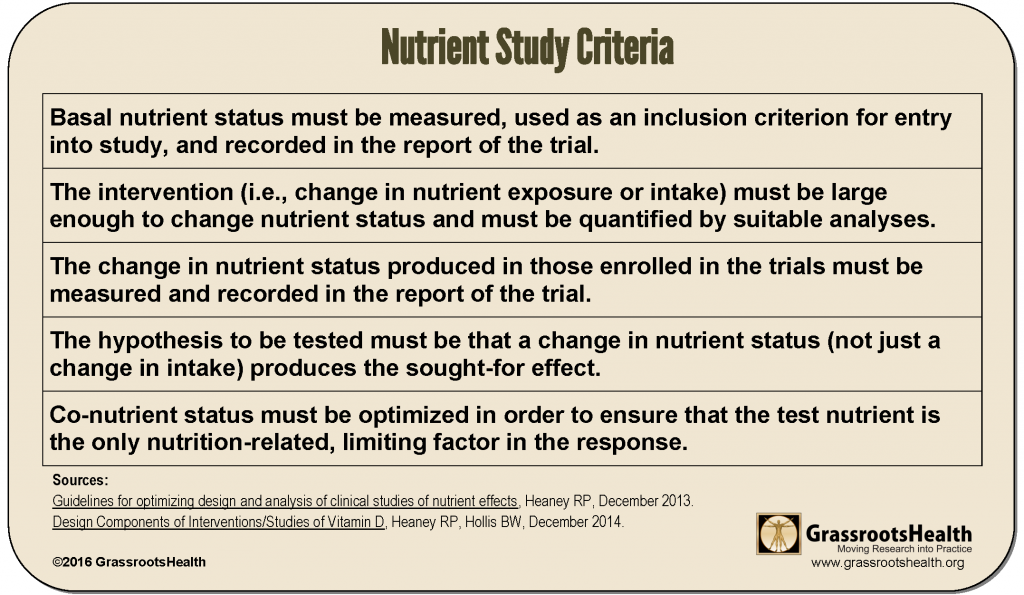
The above guidelines can be translated as follows to make them specific to vitamin D; ask yourself along the way if the vitamin D study you are questioning (such as the VITAL analysis on fracture risk) met the following criteria:
Criteria #1
a) Measure vitamin D levels [as 25(OH)D] for all participants at the beginning of the trial (this is the baseline level or basal nutrient status)
b) Baseline levels should be an inclusion criterion for participating in the study, so that the study enrolls only those with beginning vitamin D levels below the response range for the disease outcome to be observed (typically below 20 ng/ml or 50 nmol/L for most diseases)
Criteria #2
The intervention (whether it is supplementation, UVB exposure, or other) should include a sufficient dose of vitamin D to raise vitamin D levels among most treatment group participants into the therapeutic range (40-60 ng/ml or 100-150 nmol/L for many conditions)
Criteria #3
Vitamin D levels must continue to be measured and recorded at time points during the trial, and at the end of the trial
Criteria #4
a) The hypothesis should be that increased vitamin D levels into the therapeutic range (40-60 ng/ml for many conditions) will produce the specified effect (less disease, reduced symptoms, etc.)
b) The vitamin D level, not just the vitamin D dose, must be considered in the analysis
Criteria #5
Co-nutrients for vitamin D should be optimized as well; for vitamin D studies, these would include calcium, K, and magnesium among others. (Calcium levels and urine calcium/creatinine levels can also be measured at the same time points as vitamin D levels for safety.)
Other Important Questions to Ask Specific to Vitamin D Studies
Dosing Frequency
Vitamin D RCTs should avoid bolus dosing (doses given monthly or longer). Vitamin D given on a daily or weekly basis (and in the form of vitamin D3) in doses the body can make from the sunshine (not much more than 25,000 – 50,000 IU at any given time) would better match how vitamin D is intended to be ‘received’ in our bodies. It is not possible to make 100,000 IU of vitamin D in a single day, and studies doing so are more likely to have negative findings.
Length of Study
It takes time to change nutrient levels within the body, and for that change to have an effect on disease status. For example, it can take up to 20 years for precancerous cells to develop into detectable cancer. A study that lasts only 3-5 years cannot conclusively determine that vitamin D supplementation does not prevent cancer. A study period less than or equal to 6 months of testing for chronic conditions and disease prevention could basically be considered useless.
Picking Apart the VITAL Study Analysis on Fracture Risk – Did the LeBoff Paper Meet these Criteria?
In Parts 2 and 3 of this blog series, we will present a review of the VITAL trial design for its findings on fractures, according to the nutrient study criteria above, along with a detailed breakdown of WHY each criteria is essential to providing accurate and reliable study results, especially when it comes to vitamin D.
In the meantime… what do you think? Take a look at the paper with the criteria above in mind and ask yourself – did this study meet the Heaney nutrient study criteria?…
Vitamin D is an Easily Modifiable Factor to Help Improve Disease Outcomes – What Vitamin D Level do YOU Have?
Don’t ever consider a situation too late to take steps for correcting or avoiding vitamin D deficiency. Measuring your vitamin D level and calculating a supplementation amount to help reach and maintain a target level, or taking loading doses to correct deficiency faster, could possibly make all the difference in how a current disease situation progresses. Test your level now!
Create your custom home blood spot kit by adding any of the following measurements, along with your vitamin D:
- Omega-3 Index (with or without Ratios)
- Magnesium (with or without additional Elements – copper, zinc, selenium, mercury, cadmium, lead)
- hsCRP as a marker of inflammation and HbA1c as a marker of blood sugar health, two other important factors influencing prenatal conditions
Having and maintaining healthy vitamin D levels and other nutrient levels can help improve your health and the health of your baby, now and for the future. Enroll and test your levels today, learn what steps to take to improve your status of vitamin D (see below) and other nutrients and blood markers, and take action! By enrolling in the GrassrootsHealth projects, you are not only contributing valuable information to everyone, you are also gaining knowledge about how you could improve your own health through measuring and tracking your nutrient status, and educating yourself on how to improve it.
How Can You Use this Information for YOUR Health?

Having and maintaining healthy vitamin D and other nutrient levels can help improve your health now and for your future. Measuring is the only way to make sure you are getting enough!
STEP 1 Order your at-home blood spot test kit to measure vitamin D and other nutrients of concern to you, such as omega-3s, magnesium, essential and toxic elements (zinc, copper, selenium, lead, cadmium, mercury); include hsCRP as a marker of inflammation or HbA1c for blood sugar health
STEP 2 Answer the online questionnaire as part of the GrassrootsHealth study
STEP 3 Using our educational materials and tools (such as our dose calculators), assess your results to determine if you are in your desired target range or if actions should be taken to get there
STEP 4 After 3-6 months of implementing your changes, re-test to see if you have achieved your target level(s)
You may also like
 Making RCTs Work for (or Against) Vitamin D
Making RCTs Work for (or Against) Vitamin D
 Here We Go Again (Part 3 of 3) – Did the VITAL Analysis Meet the Nutrient Study Criteria for Fracture Rates?
Here We Go Again (Part 3 of 3) – Did the VITAL Analysis Meet the Nutrient Study Criteria for Fracture Rates?
 Here We Go Again (Part 2 of 3) – Did the VITAL Analysis Meet the Nutrient Study Criteria for Fracture Rates?
Here We Go Again (Part 2 of 3) – Did the VITAL Analysis Meet the Nutrient Study Criteria for Fracture Rates?
 Randomized Controlled Trials for Nutrient Research?
Randomized Controlled Trials for Nutrient Research?